We are now Enstoa, a Consertus company. Same trusted team with deep industry expertise—with expanded capabilities to meet your capital program goals. Explore more at consertus.com
Enstoa News
Matthias Ebinger for ASHE's HFM Magazine: 'Quantifying excellence for health care facilities'
Data standardization project at Yale New Haven Health builds a foundation for better operations
It certainly did not require the COVID-19 crisis for health care facilities management professionals to appreciate the value of good data. COVID-19 did, however, demonstrate to the larger health care community that chronic underinvestment in managing building data comes at a price.
There are many reasons why health care facilities professionals are struggling with the maintenance of building data. Operating budgets are tight, and few organizations have dedicated funding for the upkeep and maintenance of reliable facilities information.
The lack of a coherent approach causes inefficiencies that last through the life cycle of an asset. It quietly drains resources out of the organization; while construction data is rich in content, it is difficult to effectively merge it into operational building datasets during project turnover. There is inconsistency not only on how to name things but, more critically, on how to break complex building systems into usable datasets.
This ambiguity makes it challenging to establish effective inspections, testing and maintenance (ITM) programs, and to meaningfully assess and manage failures and risk. Datasets required by regulators, such as life safety drawings, are often maintained separate from other master building sets and diverge over time.
Health care organizations can spend significant resources again and again to reconcile these datasets. Similarly, condition assessments or energy audits often generate data that has little or no connection to the operational data maintained by the engineering department.
Yet, even organizations that fund the upkeep of master building information struggle. Existing data, tracked in drawings, 3D models, software packages for asset management, building automation, fire alarm systems, space management or condition assessments, are not coherent. Moreover, it is time consuming to maintain and even harder to interlink.
Standardization project
In 2017, Yale New Haven Health (YNHH) started a project to standardize its facilities maintenance processes across the entire health system, funded by a multi-year capital investment. Led by Steve Carbery, YNHH’s vice president of facilities design, construction and real estate, and his team of facilities professionals, the process started with discussions on what nomenclature to use.
Like many peers in the field, YNHH is a merger of previously independent hospitals, each with its own culture, data and approaches to facilities management. The natural inclination was to leverage the framework of the health system’s largest facility to minimize conversion work. However, the team soon realized a major deficiency: the framework was not designed to carry data through programming, design, construction and commissioning into operations and maintenance.
The team at YNHH reached out to peers across the field. It found that while many health facilities management organizations had invested in homegrown approaches to organizing facilities data, there was a clear interest in the formulation of a consistent framework for the health facilities management field. A call for action during several conferences resulted in a strong response.
A Health Care Facility Data Standardization (HFDS) working group was established informally, consisting of a broad spectrum of health facilities management professionals. The American Society for Health Care Engineering (ASHE), Facility Guidelines Institute (FGI), and members of the ANSI/ASHRAE/ASHE Standard 170, Ventilation of Health Care Facilities, standing standard project committee (SSPC) working group joined and provided guidance to align the work with already existing initiatives and frameworks.
Establishing principles
Recognizing the cost associated with tracking data, the HFDS working group formulated three principles to ensure that the upkeep of facilities data would be as cost effective as possible. They were:
Define the business needs for data. The HFDS working group identified use cases that the proposed framework would need to support, including:
Benchmarking of operating cost, staffing, energy use, facilities resiliency/condition within and across the organization.
Prioritization of capital and operational resource allocation to minimize organizational risk exposure.
Optimization of existing processes for ITM, fault analysis and risk assessments, including definitions on how to best bar code health care building infrastructure.
Highlight cost of ownership and optimize use of space.
Be as lean as possible. Only data that is needed to solve a defined business problem should be tracked; all other datasets should be archived and not maintained.
Align with already existing frameworks. As a highly regulated field, health care has numerous frameworks in place that provide solid structure. The HFDS working group decided to leverage, combine and complement existing frameworks rather than creating new classifications from scratch.
Defining classifications
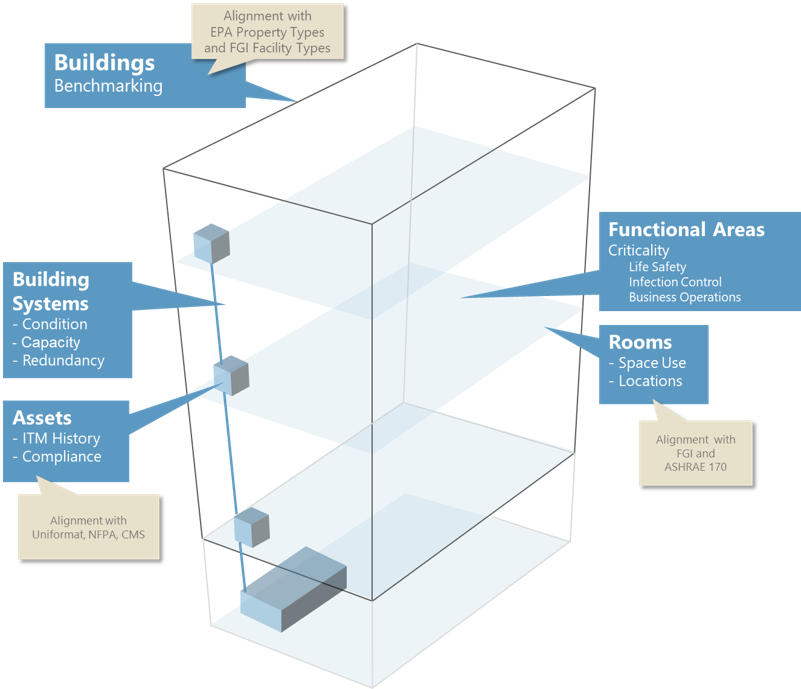
Figure 1
The HFDS working group identified the following five datasets needed by facility management to solve the identified business needs (see above):
Buildings. These are discrete physical entities composed of building systems and functional areas. Building gross square footage is a common denominator used in benchmarking of operational cost, staffing levels and energy use. Also, buildings define ownership and maintenance responsibilities.
Building systems. The term “system” is used broadly here, to not only represent utility distribution systems but also static systems such as the building envelope, barrier walls or exterior site improvements. The HFDS working group observed that few organizations capture the dataset for building systems systematically, even though it is critical to track available capacity and the areas served with their criticality, and to assess the system’s likelihood of failure by considering its condition and built-in redundancy.
Building system assets. This dataset identifies distinct assets within a system that require the documentation of inspections, testing or maintenance activities. This dataset is very granular, often containing tens of thousands of assets and detailed attribution.
Functional areas. This dataset defines spatial areas that are configured to support the needs of a health care business unit. The dataset can be used to establish criticality parameters relative to life safety, infection control, business operations and patient care.
Spaces. The last dataset defines nomenclature for spaces, either rooms enclosed with walls or areas within rooms with their own space number, such as patient bays or workstations. Inventories are used to ensure that space is used efficiently and to track the long-term cost to own and maintain these spaces.
Leveraging existing classifications. After reviewing numerous existing classifications, the HFDS working group decided to use the following frameworks as the foundation for its classification system:
Buildings. It was easy to settle on the Environmental Protection Agency’s (EPA’s) property types used in the EPA portfolio manager as categorization for buildings because they are used in ASHE’s Energy to Care benchmarking tool. In addition, the HFDS working group found that facility types defined in the FGI Guidelines align well with the definitions provided by the EPA.
Building systems. UniFormat® 2010, a framework defining the functional elements and systems of a building, published by the Construction Specification Institute, was a logical choice to use when identifying a distinct set of functional building elements and systems. UniFormat is a mature taxonomy widely used by facilities cost estimators.
Building systems assets. UniFormat 2010 was also used as the framework to define distinct assets categories. To rationalize the appropriate level of granularity for the asset categories, the HFDS working group reviewed the requirements of pertinent National Fire Protection Association (NFPA) standards; FGI Guidelines; ANSI/ASHRAE/ASHE Standard 170; ASHRAE Standard 188, Legionellosis: Risk Management for Building Water Systems, and the requirements of the Centers for Medicare & Medicaid Services and The Joint Commission. The resulting categorization schema contains 650 classes of facilities assets.
Functional areas. The FGI Guidelines contain a defined set of functional areas typically found in hospitals.
Spaces. The HFDS working group identified approximately 260 distinct space categories identified within the FGI Guidelines for hospitals.
Generating value
To assist organizations with the implementation of the new standards, and to highlight the value of their use, the HFDS working group developed several tools and use cases that are being made available by ASHE and FGI, including:
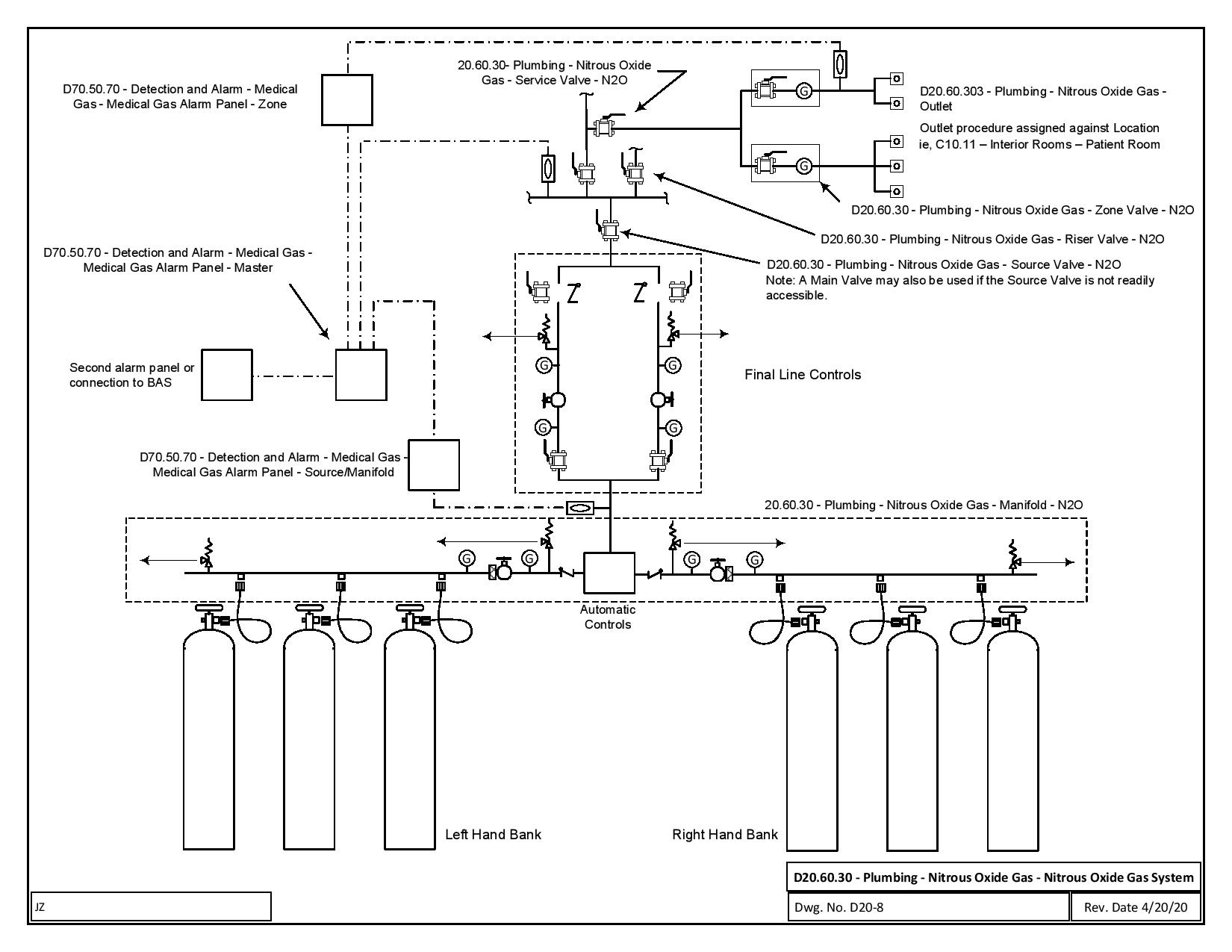
Schematic diagrams. The HFDS working group developed over 30 one-line schematics to show how building systems are compositions of specific asset classifications (see Fig. 2 below). These serve several purposes. First, they define the granularity of an asset (e.g., what should be bar coded). They also define systems and demonstrate how systems are composed of many asset categories.
Figure 2
Finally, the diagrams can be provided by facilities engineering to design engineers, contractors and commissioning agents so they can classify building systems and assets in their documentation, drawings and 3D models.
Risk management. The datasets for building systems and functional areas are most promising to provide facilities leadership with the most effective datasets. Registers for building systems and functional areas are relatively short compared to the registers of assets or spaces. When matrixing these two datasets, organizations can have an efficient tool to meaningfully manage risk, condition, capacity and investment needs.
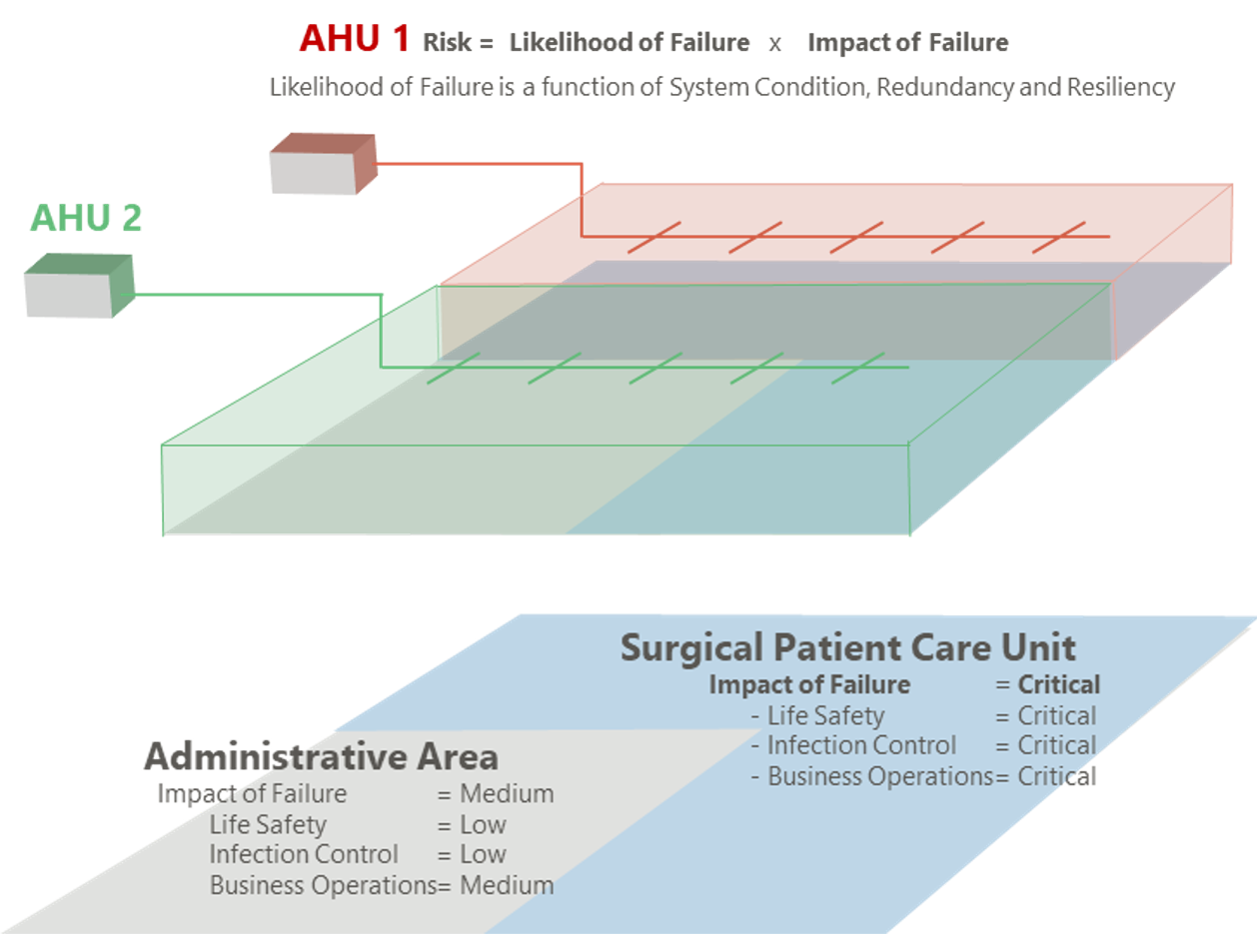
The following example demonstrates schematically the power of this approach. Fig. 3 below shows an exemplary floor plan with two functional areas: administrative and surgical patient care unit. Scores are assigned to each functional unit to rank the impact that failure of a building system would have relative to life safety, infection control, and business operations and patient care.
Figure 3
Fig. 3 interlinks these functional areas with utility distribution systems — in this example, two air handling and distribution systems. Effective risk management is now possible: with risk being a product of the likelihood of failure, multiplied by the impact, professionals now can track likelihood of failure by looking at the system’s condition, redundancy and resiliency, and multiply it with the highest impact score of the area served.
In addition, the building systems register can be used to track and benchmark operational efforts and costs. By linking requisitions for procured services, as well as work tickets from internal and external contractors, organizations can start to track and benchmark operational cost down to the system level.
Framework and future plans
The HFDS working group developed a spreadsheet with categorization schemas for all five datasets. For each dataset, the spreadsheet provides definitions and references the underlying standards and regulatory frameworks. The spreadsheet with the five data classifications and the system diagrams are available for download via the link in the Resource box on ASHE's site.
The HDFS working group is planning to use the remainder of 2020 to solicit input from facilities professionals and to test the approach with a few health systems that are working on restructuring their building data. The group expects to release in 2021 a more formal publication that will provide the results of these case studies, and highlight how organizations use the framework to manage portfolios of building assets more efficiently.
Want to learn more about how we can help standardize your data?
This article was originally published in the October 2020 edition of ASHE's HFM Magazine.
Author Bio
Matthias Ebinger is Senior Director of Digital Solutions at Enstoa. He advises healthcare organizations to optimize and digitize facilities management processes. He previously led the process engineering team within the FM department of one of the country’s largest hospital systems. Matthias studied Architecture, Public Administration and Construction Management in Germany, South Africa and the United States. He is an assistant visiting professor in the Facilities Management master’s program at Pratt Institute in New York City.
Co-authors
Stephen J. Carbery, vice president of facilities design, construction and real estate at Yale New Haven Health; Frank D. Rudilosso, director of facilities regulatory readiness at NewYork-Presbyterian Hospital; Michele Evans, environmental safety officer at the National Institutes of Health; Johnathan J. Johnson, mechanical engineer at the National Institutes of Health; George Oberlander Jr., chief engineer and director at CFS Facilities Management Inc.; and Jon Zepp, senior facilities consultant at CFS Facilities Management Inc.